







At a Glance
- Background
- Nutrition Situation
- USAID Programs: Accelerating Progress in Nutrition
- Other USAID Nutrition-Related Development Assistance
Download the nutrition profile [PDF, 345KB]
Photo credit: Kyndra Eide, Peace Corps
Background
Ghana is a mature and stable democracy, ranked in the lower-middle income status. Economic growthslowed to an estimated 5.5 percent in 2013, but has positive prospects in the long-term.1 Ghana reduced poverty from 52 percent to 28 percent over the past decade, putting it on track to reach the first Millennium Development Goal (MDG 1). Improved agricultural production has catalyzed poverty reduction, especially in the south. The agricultural sector is the largest source of income and employment and is dominated by smallholder farmers who grow both food and cash crops. Despite progress in poverty reduction, almost a quarter of Ghanaians still live below the poverty line.1
Regional disparities in poverty are apparent, with the northern region having a poverty rate nearly twice that of the south. Though there is steady progress toward reaching the health-related MDGs, the key challenge facing Ghana in terms of child and maternal health is how to accelerate progress in reducing mortality rates, which have declined slowly in contrast with the rapid progress in reducing monetary poverty and improvements on other human development indicators.
Nutrition Situation
Despite positive economic developments and poverty reduction, critical food security and nutrition challenges persist in Ghana, with the greatest burden in the three northern regions (Upper East, Upper West, and Northern Regions). As many as 1.2 million Ghanaians are considered food insecure3 and chronic undernutrition, though decreasing in the past five years, still affects about one quarter of Ghanaian children under five.4 Ghana has also reduced the prevalence of underweight in children under five from 25 percent in 1998 to 13 percent in 2011.4,5
Regional disparities in undernutrition persist: the highest stunting rates are in the Upper East, Northern, Eastern, and Central regions and the highest rates of anemia are in the Upper West and Upper East regions. Stunting is a medium-to high serious public health threat in the Feed the Future Zone of Influence, reaching 37% Northern Province. Wasting also remains a public health threat in many parts of the country, reaching close to the WHO threshold for a serious situation warranting an urgent intervention in Upper West at 9.2%.
Food insecurity, inadequate feeding practices, lack of dietary diversity, and low access to health services are among the main causes of undernutrition in children6. Micronutrient deficiencies including vitamin A and iron are a critical public health challenge with the highest burden on young children and women. The prevalence of child anemia has greatly reduced from 78 percent in 20087 to 57 percent in 2011;4 however, the rate is still above 40 percent, the WHO cutoff point for a severe public health problem.
| Ghana Nutrition Data | ||
|---|---|---|
| Population (2012) | 24.6 Million | |
| Population under 5 years of age (0-59 months, 2012) | 3.6 Million | |
| DHS 20087 | MICS 20114 | |
| Prevalence of stunting among children under 5 (0-59 months) | 28% | 23% |
| Prevalence of underweight among children under 5 (0-59 months) | 14% | 13% |
| Prevalence of wasting among children under 5 (0-59 months) | 9% | 6% |
| Prevalence of anemia among children aged 6-59 months | 78% | 57% |
| Prevalence of anemia among women of reproductive age (15-49 years) | 59% | n/a |
| Prevalence of thinness among women of reproductive age (15-49 years) | 9% | n/a |
| Prevalence of children aged 0-5 months exclusively breastfed | 63% | 46% |
| Prevalence of breastfed children aged 6-23 months receiving a minimum acceptable diet | 27% | 31% |
National Nutrition Policies
Ghana established the Cross-Sectoral Planning Group (CSPG), a multi-stakeholder platform under the National Development Planning Commission. The CSPG is working to introduce a nutrition baseline and identify trends in nutrition financing. The CSPG played an active role in the development of the 2014 National Nutrition Policy, which seeks to: (a) reposition nutrition as a cross-cutting issue, (b) facilitate integration and mainstreaming of nutrition into all national development efforts; (c) provide the framework for nutrition-specific and nutrition-sensitive services and interventions; (d) guide the implementation of high-impact interventions; and (e) strengthen sectoral capacity for the effective delivery of these interventions.
In 2011, Ghana joined the Scaling Up Nutrition (SUN) Movement, a global movement uniting national leaders, civil society, bilateral and multilateral organizations, donors, businesses, and researchers in a collective effort to improve nutrition. USAID is the donor convener for SUN in Ghana. Ghana’s priorities under SUN include increasing government nutrition funding, prioritizing nutrition among key stakeholders, and improving the measurement of nutrition indicators.8
Ghana participates in the African-led Comprehensive Africa Agriculture Development Program (CAADP), which brings together governments and diverse stakeholders to reduce hunger and poverty and promote economic growth through agricultural development. With the CAADP, Ghana revised its 2002 Food and Agricultural Sector Development Policy (FASDEP) to involve the private sector and farmer-based organizations in agricultural policy implementation.
Ghana is also a part of the New Alliance for Food Security and Nutrition, a partnership between African heads of state, corporate leaders, and G8 members to accelerate implementation of CAADP strategies. In Ghana the New Alliance goals are to: to generate greater private investment in agricultural development, scale innovation, achieve sustainable food security outcomes, reduce poverty, and end hunger.
USAID Programs: Accelerating Progress in Nutrition
| Highlighted Bilateral Nutrition Projects in Ghana | ||||
|---|---|---|---|---|
| Project Name | Year Awarded | End Date | Objective(s) | |
| Systems for Health | 2014 | 2019 | To reduce underweight, stunting, and anemia of women and children in five regions in Ghana. | |
| Resiliency in Northern Ghana (RING) | 2014 | 2018 | RING is focused on poverty reduction and improving the nutritional status in vulnerable households | |
| SPRING | 2014 | 2017 | To reduce stunting and anemia among under fives in three regions of ZOI. | |
Feed the Future Progress
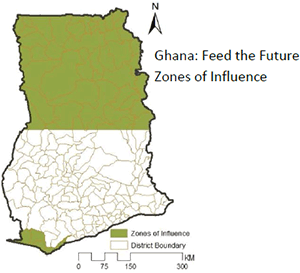
Ghana’s Feed the Future initiative focuses on the northern half of the country because of that region’s lower food security levels and higher poverty rates. Ghana’s Feed the Future strategy addresses three key intermediate results: increased competitiveness of major food value chains; improved resilience of vulnerable communities and households; and improved nutritional status for women and children. The Feed the Future strategy strongly links agricultural production with income growth, and is focused on improved production methods, reducing post-harvest losses, removing gender constraints, improving agricultural policy, and expanding credit via a predominantly private-sector led approach.
USAID/Ghana: Feed the Future Targets for 2015
- Help an estimated 860,000 vulnerable Ghanaian women, children and family members—mostly smallholder farmers—escape hunger and poverty.
- Reach more than 324,000 children with services to improve their nutrition and prevent stunting and child mortality.
- Significant numbers of additional rural populations will achieve improved income and nutritional status from strategic policy engagement and institutional investments.
The existing Feed the Future value chain project, the Agricultural Development and Value Chain Enhancement (ADVANCE II) project, is working with smallholder farmers in the north in the maize, rice, and soy value chains to link them to markets, finance, inputs, equipment and information through larger commercial farmers and traders. The Resiliency in Northern Ghana (RING) project, focused on rural, vulnerable farm families, will co-locate with ADVANCE and other USAID activities to increase resilience by improving livelihoods and nutritional well-being, aiming to improve the nutritional status of women and children less than two years old.
RING interventions aim to diversify livelihoods, increase household income, increase access to credit and community safety nets, and improve output from smallholder agricultural activities, with a strong focus on local governance. It is estimated that there will be at least a 20 percent reduction in stunting, wasting, and underweight among children under five by 2017.
Other ongoing projects address health systems improvement (Focus Region Health) and BCC strategies (Ghana Behavior Change Support Project) but they are outside of the Feed the Future ‘zones of influence.9
Active Global Nutrition Mechanisms
In early 2014 the Mission is investing in the SPRING (Strengthening Partnerships, Results, and Innovations in Nutrition Globally) Project. SPRING will focus on averting wasting and stunting among 60,000 children through supporting work in the community-based management of acute malnutrition; infant and young child feeding; distribution of micronutrient powders to children under the age of five, promotion healthy behaviors related to water, sanitation, and hygiene, aflatoxin prevention and control, and anemia prevention and control. The project will work at the District and Regional levels in Northern and Upper East Regions and will leverage capacity of the Ghana Health System and the resources of complementary USAID investments.
Under USAID’s flagship Maternal and Child Health Integrated Program (MCHIP), pre-service education is being strengthened in twenty-eight midwifery schools, ten community health nursing schools, one public health school and one medical assistant school by: 1) ensuring competency of tutors, preceptors and new graduates (in malaria, HIV, tuberculosis, family planning, nutrition, and maternal and newborn health); 2) equipping skills labs; and 3) introducing e-learning.
Through GAIN (Global Alliance for Improved Nutrition), USAID/Washington is supporting analyses to identify the ways the use of local foods can be optimized to promote health and nutrition in the thousand day window, from pregnancy to a child’s second birthday. These two analyses, Optifood and a Focused Ethnographic Study, are expected to produce findings that will be used to inform programming in nutrition during the coming years.
Other USAID Nutrition-Related Development Assistance
PEPFAR Ghana’s key strategic priorities include prevention of HIV in persons engaged in high-risk behaviors; reducing HIV transmission from key populations to the general population; and providing comprehensive prevention, care, and access to treatment for those infected, their partners, and their families. Nutrition support is also provided in this continuum of care and includes providing therapeutic supplementation for low-BMI patients commencing ART (antiretroviral therapy).10
The NACS Program (nutrition assessment, counseling and support) is a key component of the MOH’s and GHS’s commitment to integrate nutrition into policies, programs, and health delivery systems, and scale up quality nutrition services. In 2006, the MOH and GHS launched national guidelines on Nutritional Care and Support of People Living with HIV/AIDS (PLHIV), as the first step in integrating NACS into HIV services.
In 2010/2011, GHS piloted the NACS approach in 11 HIV care and treatment centers and plans to scale up the rollout of NACS to an additional 29 facilities; covering more than 200 clinicians and care providers. In 2011, 3,396 HIV clients received NACS services out of which 268 clinically malnourished clients received therapeutic food at 11 sites under the new ‘food by prescription’ program.10
Ghana joined the Committing to Child Survival: A Promise Renewed campaign in 2012, and pledged to reduce under-five mortality to 20 or fewer deaths per 1,000 live births by 2035 by reducing the leading preventable causes of child mortality, including undernutrition. To view the country action plan for ending preventable child and maternal deaths in Ghana, please see the Acting on the Call 2014 report.
References
- World Bank Ghana Country Overview.
- Feed the Future Ghana Country Profile..
- Ghana Ministry of Food and Agriculture, Northern Region Agricultural Development Unit website.
- Ghana Multiple Indicator Cluster Survey 2011. GSS, GHS, UNICEF, UNFPA, Japan Official Development Assistance, and USAID.
- Ghana Statistical Service (GSS) and Macro International Inc. (MI). 1999. Ghana Demographic and Health Survey 1998. Calverton, Maryland: GSS and MI.
- Ghana Nutrition Profile. Nutrition and Consumer Protection Division, FAO, 2009.
- Ghana Demographic and Health Survey 2008.Accra, Ghana: GSS, GHS, and ICR Macro.
- Scaling Up Nutrition: Ghana.
- Feed the Future Ghana Strategy Paper and Landscape Analysis Mission Report.
- Ghana PEPFAR Operation Plan Report, 2012.
Comment
Make a general inquiry or suggest an improvement.